The Impact of Visual Cues to Improve Perioperative Hand Hygiene Compliance


Background
- In an acute care hospital with a specialized unit for orthopedic surgeries; Hand Hygiene Compliance (HHC) is monitored in all inpatient and outpatient units except for the peri-operative areas.
- There is minimal evidence on the applicability of WHO’s best practice guidelines on the HHC for the non-scrubbed members of the perioperative team.
- According to the Center for Disease Control and World Health Organization, HHC can decrease the prevalence of surgical site infection and other hospital acquired infections (Speth, 2023).
- Studies supports that a sustainable and significant increase in HHC can be achieved through the combination of any of the following visual cues: male/female eyes, signage, increased visibility, and towel presentation (Ford E, 2014; King D, 2016; Nevo I, 2010; Owings A, 2022).
- WHO introduced the five moments of HH in 2019, but it was considered inapplicable to the perioperative environment (Smith et al., 2020). The application of the five moments of the HH to the Operating Room may help set expectation for HH practices and thus decrease the chances of healthcare worker related cross contamination (Lee, 2019; Smith et al., 2019).


Purpose
The purpose of this QI project is to determine whether visual cues increase hand hygiene compliance in non-scrubbed OR members.
Methods
Design: Quality Improvement (QI) Project in an acute care orthopedic operating room.
Sample: All operating room staff in the non-scrubbed role.
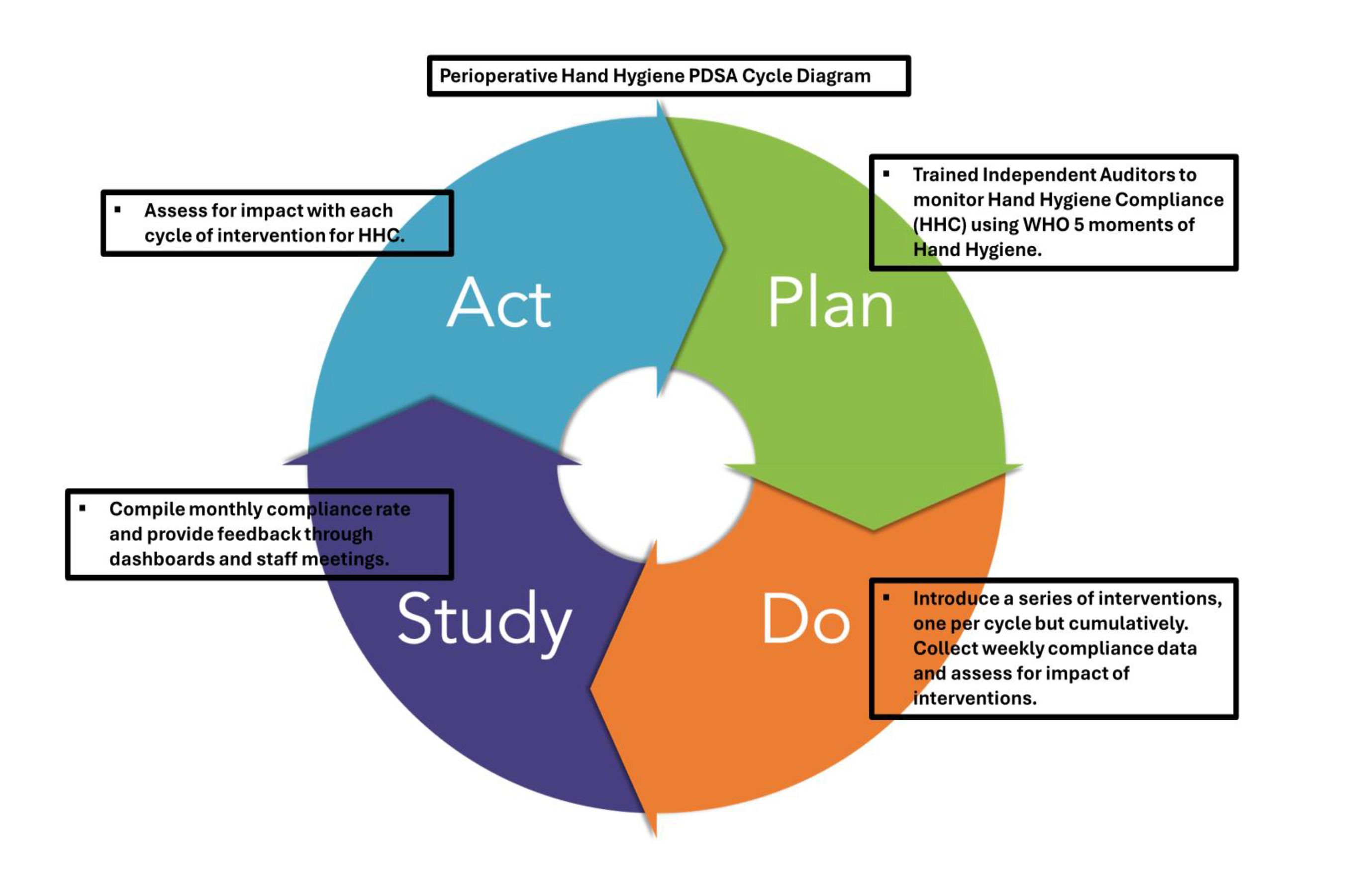
Theoretical Framework: The Plan-Do-Study-Act (PDSA) method was used to evaluate the impact of education, and visual cues on Hand Hygiene over 6 months.

Demographic:
The auditors collected demographics such as role and time of day. Roles were defined as job title such as Anesthesia team, Surgical team, Registered Nurse and Operating Assistive Personnel.
Tool Creation:
An audit tool was created using the WHO recommended 5 moments of Hand Hygiene (HH) as applicable to the Operating room setting and the existing audit tool for HH monitoring on inpatient units within the institution (Lee T, 2019, WHO, 2019).
The audit tool was used to collect monthly hand hygiene compliance report data by trained personnel.
The five criteria/ HH opportunities identified by WHO are:
- Criteria One: Upon entering the OR doors, excludes patient transfer since hand hygiene should have been done prior.
- Criteria Two: Before any assessment, procedure, or patient care where contact is made with non-intact skin or mucus membranes, insertion or disruption of invasive device, medication administration.
- Criteria Three: After any potential body fluid exposure.
- Criteria Four: After exiting the OR doors, excludes patient transfer since hand hygiene should have been done after touching patient's bed/surrounding.
- Criteria Five: After contact with patient surroundings. When a patient is not touched, after contact with inanimate objects such as door etc.


Interventions:
- First Intervention: An assessment of the current work environment was performed followed by the installation of additional Purell stations to ensure ease of application.
- Second Intervention: An education session was provided to all perioperative staff detailing the importance of hand hygiene and the 5 moments of Hand Hygiene in perioperative area.
- Third Intervention: Visual Cues were installed on all sanitizing station.
Results:
- 179 observations were collected between July and December 2023.
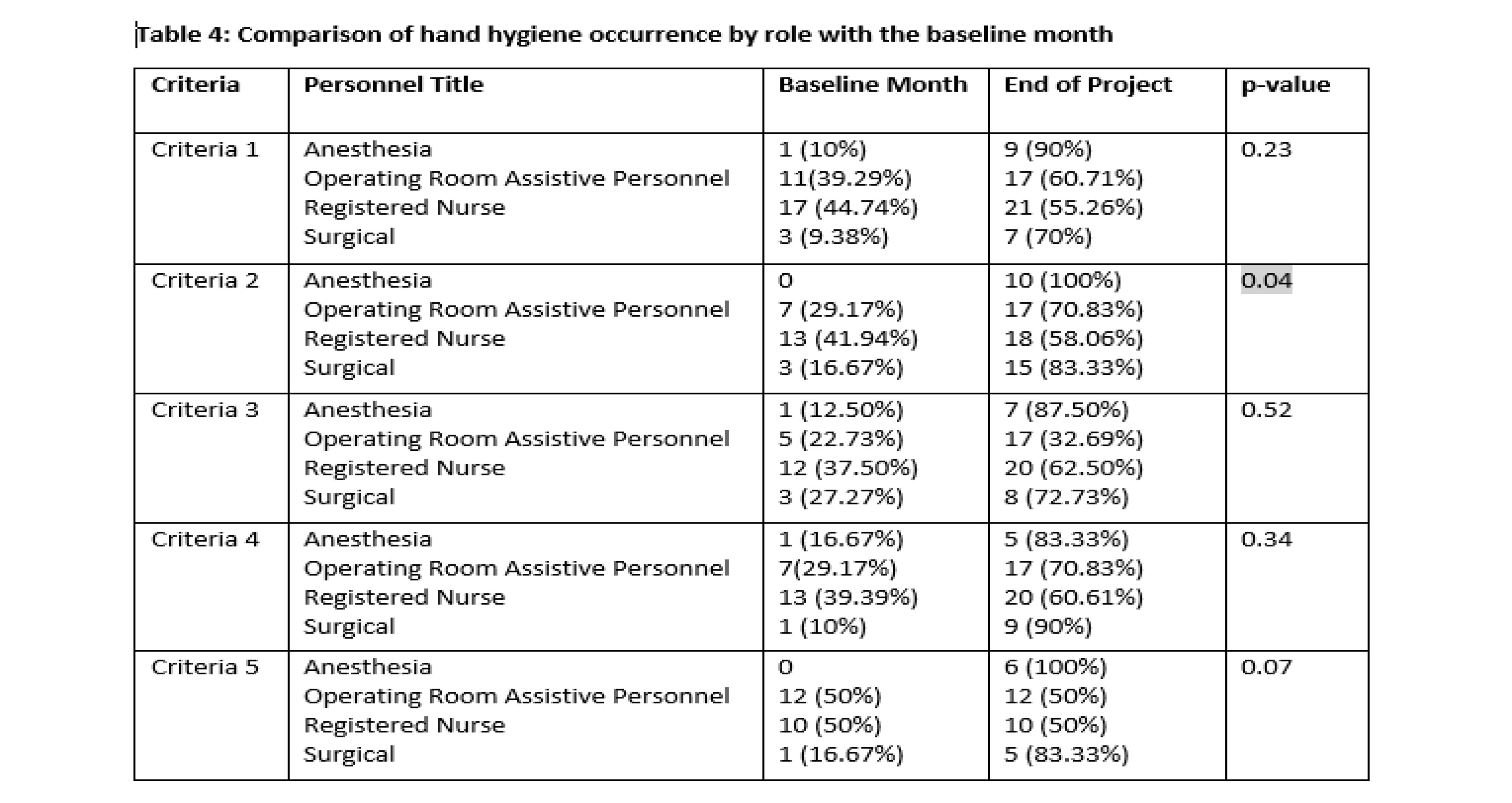
- Operating Room (OR) Assistive Personnel and Registered Nurses (RN) had greater odds of intervention association on hand hygiene compliance than surgical team in criteria 1, 3, 4 and criteria 5 with statistical significance.
- When comparing post intervention data to baseline data, Criteria 2 showed statistically significant improvement in HHC for all roles, with the greatest HHC increases: Anesthesia increased from 0% to 100%, OR Assistive Personnel from 29% to 70.83%, RNs from 41% to 58.06% and Surgical Team from 16% to 83.33%.

Discussion
- The PDSA method proved most successful for measuring compliance because it allowed for changes in intervention to achieve the sustainable compliance rate.
- A focus on HH practices with the OR suite and outside the scrubbed role brings with it challenges.
- The implementation of this HH initiative was successful with organizational and leadership buy-in.
- Feedback was solicited from participants at staff meetings, huddles and via email on barriers to HHC.
- Individual and professional accountability is crucial to ensure a sustained change in hand hygiene practice.
- Limitations of this study are related to the convenience sampling method and the role of the primary research as a nursing leader. This is evident in the greater odd of hand hygiene compliance post intervention with the disciplines reporting to nursing versus provider group.
Conclusion
- The combination of education and visual cues proved most effective in increasing HHC; however, a sustained compliance rate requires leadership involvement and a focus on accountability amongst team members.
- The findings were consistent with literature in what it takes to change the culture and sustain HH practices.
References
Ford E, B. B. (2014). Increasing hand washing compliance with a simple visual cue. American Journal of Public Health, 104(10), 1851-1856.
King D, V. I.-T. (2016). Priming hand hygiene compliance in clinical environment. Health Psycology, 35(8), 96-101.
LaMorte, W. (2019). Behavioral change models: The theory of planned behavior. https://sphweb.bumc.bu.edu/otlt/mph-modules/sb/behavioralchangetheories/BehavioralChangeTheories3.html
Nevo I, F. M.-T. (2010). The efficacy of visual cues to improve hand hygiene compliance. Simulation in healthcare, 5(6), 325-331.
O’Boyle,C., Henly, S., and Larson, E. (2001). Understanding adherence to hand hygiene recommendations: The theory of planned behavior. American Journal of Infection Control, 29(6), 352–360. https://doi.org/10.1067/mic.2001.18405
Owings A, C. L. (2022). Improving visitors' hand hygiene compliance in a pediatric oncology unit. American Journal of Infection Control(50), 724-728.
Paul E, K. M. (2019). Sleep safe in clean hands: Improving hand hygiene compliance in the operating room through education and increased access to hand hygiene products. American Journal of Infection Control(37), 504-508.
Speth, J. (2023). Guidelines in Practice: Hand Hygiene. AORN Journal, 118(2), 101–108. https://doi-org.libdb.fairfield.edu:8443/10.1002/aorn.13964
Voight, P., Fuller, M., & McKean, K. (2022). The Perioperative Steering Committee as an Accountable Infrastructure to Enable and Sustain Change. AORN Journal., 116(1), 23–33. https://doi.org/10.1002/aorn.13707
Acknowledgements
To God be all the glory, honor, and praise for the inspiration, guidance and wisdom granted towards the successful completion of this project.
Special thanks to my family for their support and patience.
Thank you to my advisors Dr. Sally Gerard and Dr. Cynthia Bautista
Thank you to Stamford Health and the Hospital for Special Surgery at Stamford Collaborative Team

Presented at:

